|
|
||
| Материалы Международного межуниверситетского семинара по диагностической и терапевтической радиологии Минск, 20-21 октября 2003 года |
Biliary Malignancies: Multislice-CT or MRI?
Prof. Wolfgang Schima, MD
Department of Radiology, Univ. of Vienna, Austria.
(Радиология в медицинской диагностике [современные технологии]
2003: 91-94)
Abstract.
Cholangiocarcinoma is the most common malignant bile duct and the second most
common primary malignant tumor in the liver. It can be classified as intrahepatic
(peripheral) or extrahepatic. Extrahepatic cholangiocarcinomas originate most
often from the main hepatic duct and confluence (referred to as Klatskin tumor).
The patients usually present with jaundice because of biliary obstruction. Prognosis
of hilar cholangiocarcinoma is poor, because most tumors are unresectable at
the time of diagnosis. Surgical exploration should only be undertaken, when
there is a potential for curative resection shown by radiologic imaging.
ERCP demonstration of Klatskin tumors is often incomplete due to incomplete
filling of bile ducts peripheral to the stenosis. MR imaging and helical CT
are the methods of choice in the diagnosis and staging of hilar cholangiocarcinoma.
MR cholangiography in conjunction with MRI and MRA provides information of tumor
size, bile duct involvement, and vascular compromise, and thus, resectability
of the tumor. Multi-phasic contrast-enhanced thin-section helical CT may show
Klatskin tumors with a sensitivity of up to 100%. Tumors are better seen on
arterial-dominant phase than on portal venous phase scans (sensitivity, 100%
vs. 86%). However, single slice CT is not accurate for assessing resectability
(accuracy, 60%), because proximal tumor extent is largely underestimated. Preliminary
experience with multi-slice CT indicates that the extent of bile duct involvement
may be better displayed due to multi-planar imaging capabilities. Curved planar
reconstruction of multi-slice CT data sets along the portal vein and the bile
ducts reveal tumor involvement.
Intrahepatic cholangiocarcinomas have a non-specific imaging appearance. Because
of abundant fibrous stroma, they exhibit little contrast enhancement during
CT or MRI scanning in the early phase with delayed accumulation of contrast
material. Although not pathognomonic, the presence of bile duct dilatation within
the tumor and retraction of the liver capsule adjacent to the tumor are suggestive
of the diagnosis.
In conclusion, the role of contrast-enhanced MRI with MR cholangiography and
multi-slice CT in the detection and preoperative staging of cholangiocarcinoma
is emphasized.
Introduction.
A number of examination techniques are available for evalation of the biliary
tracts. Transabdominal ultrasound is the primary non-invasive technique for
assessing patients with suspected bile duct and gallbladder pathology. An experienced
examiner can assess intrahepatic and extrahepatic bile ducts in the vast majority
of patients, regardless of the body habitus. The presence of dilated bile ducts
as an indicator of biliary obstruction can be reliably seen. However, the underlying
etiology of obstruction in the distal common bile duct may be obscured at ultrasound.
MR cholangiopancreatography (MRCP) is now the established non-invasive method
of choice for evaluation of biliary obstruction. MRCP is performed with heavily
T2-weighted pulse sequences during one breathhold or with free breathing. Usually,
the biliary tract is first localized with radially oriented single-shot thick-slab
images. Then a multi-slice HASTE pulse sequence in coronal/oblique plane provides
thin (3–5 mm) source images of the biliary and pancreatic duct system. Axial
HASTE source images may help in the differentiation between intraluminal ductal
stones and air bubbles due to aerobilia, because intraductal stones may be surrounded
by fluid, whereas air bubbles float on the fluid in the non-dependent portion
of the bile duct.
Computed tomography has been the standard imaging technique to evaluate liver
and pancreatic tumors in many institutions. However, it has two major limitations
with regard to bile duct imaging. Bile duct stones may not be seen, unless calcified
and bile duct tumors are difficult to differentiate. However, the evolution
of multi-slice CT has brought major advances in bile duct images with CT. The
acquisition of a MSCT data sets allows 3D-reconstruction of the scanned volume
in coronal or oblique orientation which is particularly helpful for visualization
of the biliary system.
Cholangiocarcinoma.
Cholangiocarcinomas arise from any portion of the intrahepatic or extrahepatic
bile duct epithelium. They are classified as intrahepatic (peripheral) cholangiocarcinoma
or extrahepatic cholangiocarcinoma. Intrahepatic cholangiocarcinomas are the
second most common primary malignancy of the liver. Extrahepatic cholangiocarcinomas
originate most often from the main hepatic duct and confluence (often referred
to as Klatskin tumor) and become clinically apparent because of biliary obstruction.
Klatskin tumor.
Hilar cholangiocarcinomas (Klatskin tumors) are categorized according to the
Bismuth classification (Fig. 1): a type I tumor involves the
main hepatic duct below the bifurcation, a type II tumor affects the main hepatic
duct bifurcation. A type III tumor involves segmental ducts beyond the primary
hepatic duct bifurcation in one liver lobe (type IIIa: right lobe, type IIIb:
left lobe). Type IV tumors involve segmental ducts in both liver lobes. Prognosis
of hilar cholangiocarcinoma is poor, with most of the tumors being unresectable
at the time of diagnosis. Thus, surgical exploration should only be undertaken,
when there is a potential for curative resection shown by imaging.
|
Radiologic evaluation.
Diagnosis of Klatskin tumors was a domain of ERCP, which may show of bile duct
involvement and histologic proof. However, ERCP demonstration of bile duct anatomy
is often incomplete due to incomplete ductal filling. MR imaging and helical
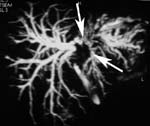
CT are useful in diagnosis and staging of Klatskin tumors. MRCP in conjunction
with contrast-enhanced MRI and MRA allows assessment of tumor size, bile duct
involvement (Fig. 2), and vascular infiltration, which is crucial
for assessment of resectability. Contrast-enhanced thin-section helical CT may
show Klatskin tumors with a sensitivity of up to 100%. Tumors are better seen
on arterial-dominant than on portal venous phase scans (sensitivity 100% vs.
86%). However, single-slice helical CT is still inaccurate for assessing resectability
(accuracy, 60%), because proximal tumor extension is underestimated. Preliminary
experience with multi-slice CT indicates that tumor extension may be better
displayed due to 3D-imaging capabilities. Curved planar reconstructions along
the main, right, and left portal vein and along the intrahepatic bile ducts
show the extent of tumor involvement more precisely. In contrast to “conventional”
axial images, they reveal a “pseudosurgical” view of the tumor growth pattern.
|
|||
Intrahepatic (peripheral) cholangiocarcinoma.
Peripheral cholangiocarcinoma is a primary adenocarcinoma of the liver arising
from the epithelium of the small bile ducts. Intrahepatic cholangiocarcinomas
have a non-specific imaging appearance. Because of the presence of abundant
fibrous stroma, these tumors most often show little contrast enhancement at
CT or MRI scanning in the early phase, but delayed accumulation of contrast
material. Although being non-specific, the presence of bile duct dilatation
within the tumor and liver capsule retraction adjacent to the tumor are suggestive
of the diagnosis .
Conclusion.
In conclusion, detection and accurate staging of Klatskin tumor is improved
by multi-phasic helical CT scanning and MR imaging. Curved-planar reconstructions
from multi-slice CT data sets with thin collimation may further improve our
ability to diagnose vascular involvement. MR cholangiography in conjunction
with contrast-enhanced MRI provide 3D-images of the biliary tracts that facilitate
planning of surgery or guide palliative drainage.
References:
1. Bismuth H, Nakache R, Diamond T. Management strategies in resection for hilar
cholangiocarcinoma. Ann Surg 1992, 215: 31
2. Fulcher AS, Turner MA. HASTE MR cholangiography in the evaluation of hilar
cholangiocarcinoma. AJR 1997; 169: 1501
3. Tillich M, Mischinger, H-J, Preisegger K-H, Rabl H, Szolar DH. Multiphasic
helical CT in diagnosis and staging of hilar cholangiocarcinoma. AJR 1998; 171:
651
4. Nino-Murcia M, Jeffrey RB, Beaulieu CF, Li KCP, Rubin GD. Multidetector CT
of the pancreas and bile ducts: value of curved planar reformations. AJR 2001;
176: 689
5. Sahani S, Saini S, Pena C, et al. Using multidetector CT for preoperative
vascular evaluation of liver neoplasms: technique and results. AJR 2002; 179:
53
6. Lee JW, Han JK, Kim TK, et al. CT features of intraductal intrahepatic cholangiocarcinoma.
AJR 2000; 175: 721
7. Soyer P, Bluemke DA, Sibert A, Laissy JP. MR imaging of intrahepatic cholangiocarcinoma.
Abdom Imaging 1995; 20: 126
8. Choi BI, Han JK, Shin YM, Baek SY, Han MC. Perpheral cholangiocarcinoma:
comparison of MRI with CT. Abdom Imaging 1995; 20: 357
9. Zhang Y, Uchida M, Abe T, Nishimura H, Hayabuchi N, Nkashima Y. Intrahepatic
peripheral cholangiocarcinoma: comparison of dynamic CT and dynamic MR. J Comput
Assist Tomogr 19999; 23: 670
|
|
|||||||