|
|
||
Hemifacial neuropathy as a result of osteophyte.
Sergey V. Sheleg1, M.D., Ph.D, Sergey A. Khoruzhik2, M.D., Evgeny A. Korotkevich3, M.D., D.Sc., Yury G. Shanko3, M.D., Ph.D., Arnold F. Smeyanovich3, M.D., D.Sc.
1Center for Biologics Evaluation and Research, U.S. Food and Drug Administration, Bldg. 29A, Rm 2C-11, 8800 Rockville Pike, Bethesda, MD 20892, U.S.A. Phone: (301) 827 1823, Fax: (301) 827 1825. 2Radiology Division, N.N. Alexandrov Research Institute of Oncology and Medical Radiology, Minsk, P.O. Lesnoy-2, 223052, Republic of Belarus. 3Research Institute of Neurology, Neurosurgery, and Physiotherapy, Filatova St. 9, Minsk, 220026, Republic of Belarus.
Key words: hemifacial neuropathy, multi-slice computerized tomography, facial nerve plasty
We report the case of a 58-year-old man with non-Hodgkin lymphoma of the stomach
who presented with the symptoms of left-side facial palsy manifesting for three
months. No generalized skeletal disease which may cause the hemifacial neuropathy
and respiratory viral infections was evident. CSF analysis did not show lymphoma
cells. The patients did not complain of tinnitus, vertigo, or hearing loss.
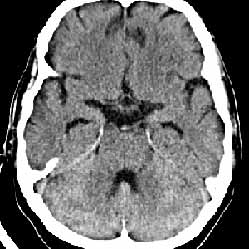
No brain metastases from non-Hodgkin lymphoma could be detected by contrast-enhanced
axial computerized tomography (Figure, right).
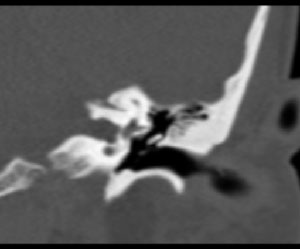
Multi-slice computerized tomography (MSCT) of the brain with 2-dimensional reconstruction
showed an osteophyte of the upper wall of the left auditory meatus (size 2.4
2.2 mm) (Figure, left).
|
|||||
We performed surgical extracranial reinnervation of the facial nerve by means
of single-step plasty of the facial nerve with hupoglossal nerve trunk. Three
months after the surgery, partial restoration of the left facial nerve function
was established.
Manni et al.1 reported a case of the eighth cranial nerve dysfunction as a result
of hyperostosis cranialis interna with the presence of normal audiogram and
unilateral facial nerve paralysis.
The above case is the only one we are aware of in which a little osteophyte
in the left auditory meatus is accompanied by left facial nerve paralysis without
hearing loss and vertigo. MSCT with 2-dimensional reconstruction may provide
superior imaging of this kind of pathology.
References:
1. Manni JJ, Huygen PL, Noten JF, Kuijpers W: Eighth cranial nerve dysfunction
in hyperostosis cranialis interna. Acta Otolaringol 11:75-82, 1992.
|
|
|||||||